Melanoma doesn’t always look like a scary mole. Sometimes it’s a tiny spot that doesn’t fade. Other times, it’s a bump that bleeds slightly after brushing against your shirt. The problem? Most people ignore it-until it’s too late. In 2025, the American Cancer Society reported that when melanoma is caught early, the 5-year survival rate is over 99%. But if it spreads, that number drops to just 32.1%. That’s not a small gap. That’s life or death. And today, the tools we have to catch it early-and treat it if it spreads-are changing faster than ever.
What Melanoma Really Looks Like (And Why You Can’t Rely on the ABCDE Rule Alone)
The ABCDE rule-Asymmetry, Border irregularity, Color variation, Diameter larger than 6mm, Evolving size or shape-is still taught in medical schools. But it’s not enough. Studies show primary care doctors using only visual inspection miss between 30% and 40% of melanomas. Why? Because melanoma doesn’t always follow the rules. Some are tiny, under 3mm. Others look like a regular freckle. A lot of them appear on skin you don’t check often: the scalp, under nails, between toes, even the back of the ear.
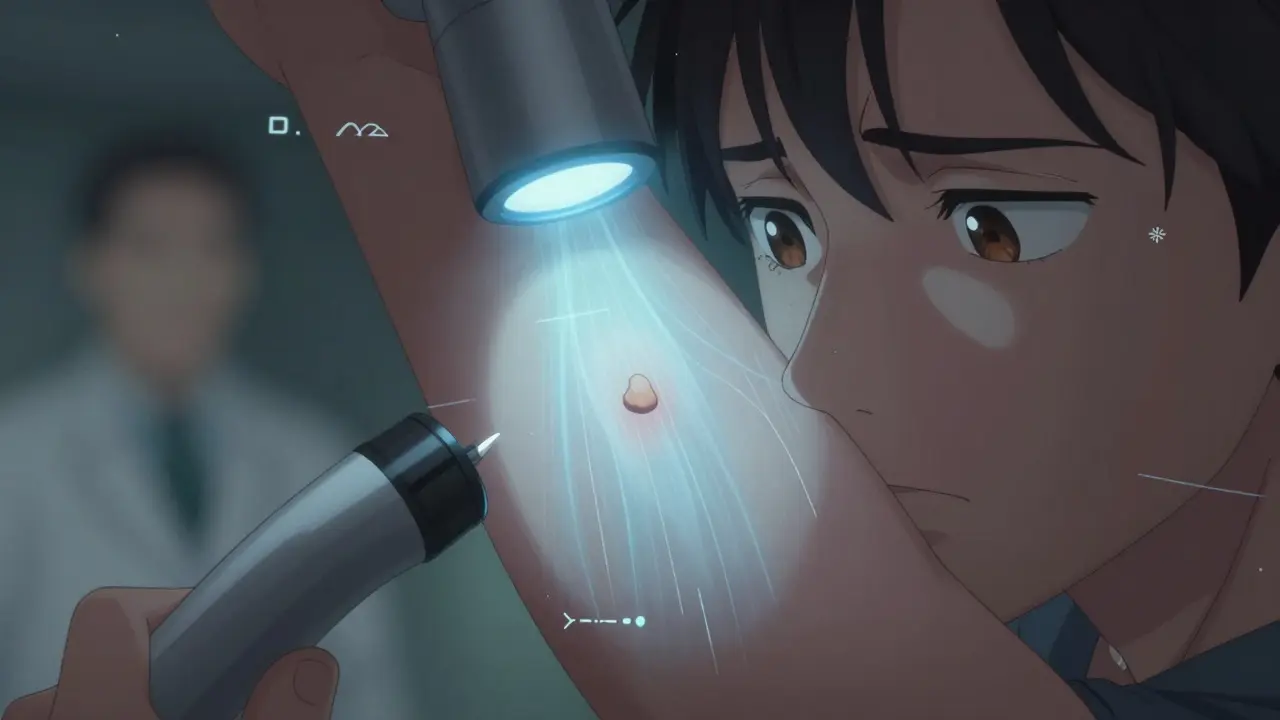
That’s why dermoscopy is now standard. It’s a handheld device with a magnifying lens and polarized light that lets doctors see beneath the skin’s surface. Dermatologists use it to spot patterns invisible to the naked eye: blue-white veils, irregular streaks, or regression areas. But even dermoscopy has limits. It’s only as good as the person using it. And not every clinic has a dermatologist on site.
AI Is Now a Second Pair of Eyes in the Exam Room
In 2024, the FDA cleared the DermaSensor, a handheld device that shines near-infrared light on a skin spot and measures how the light scatters. It doesn’t replace the doctor-it gives the doctor better data. In trials, primary care providers using DermaSensor increased their accuracy by 11%. But here’s the catch: its specificity is only 26-40%. That means for every 100 people it flags as suspicious, 60-74 are false alarms. More biopsies. More anxiety. More cost.
That’s where AI models like SegFusion come in. Developed at Northeastern University and published in March 2025, it combines two neural networks: one to outline the exact shape of a lesion, and another to classify it. It’s trained on over 100,000 images from the ISIC archive, with special adjustments to balance datasets-because melanoma only makes up 1.8% of most image libraries. The result? 99% accuracy, 95% sensitivity. That’s better than most human dermatologists. And it’s being tested in clinics across the U.S. and Europe.
But AI isn’t perfect. It struggles with darker skin tones. A March 2025 JAMA Dermatology study found existing models are 12-15% less accurate on Fitzpatrick skin types IV-VI. That’s not a small error. That’s dangerous. Researchers are now training models on diverse datasets, but progress is slow. If you have darker skin, don’t assume an AI tool is flawless. Always ask your doctor: Was this image reviewed by someone trained on diverse skin tones?
Wearable Patches and Full-Body Scanners: The Future Is Already Here
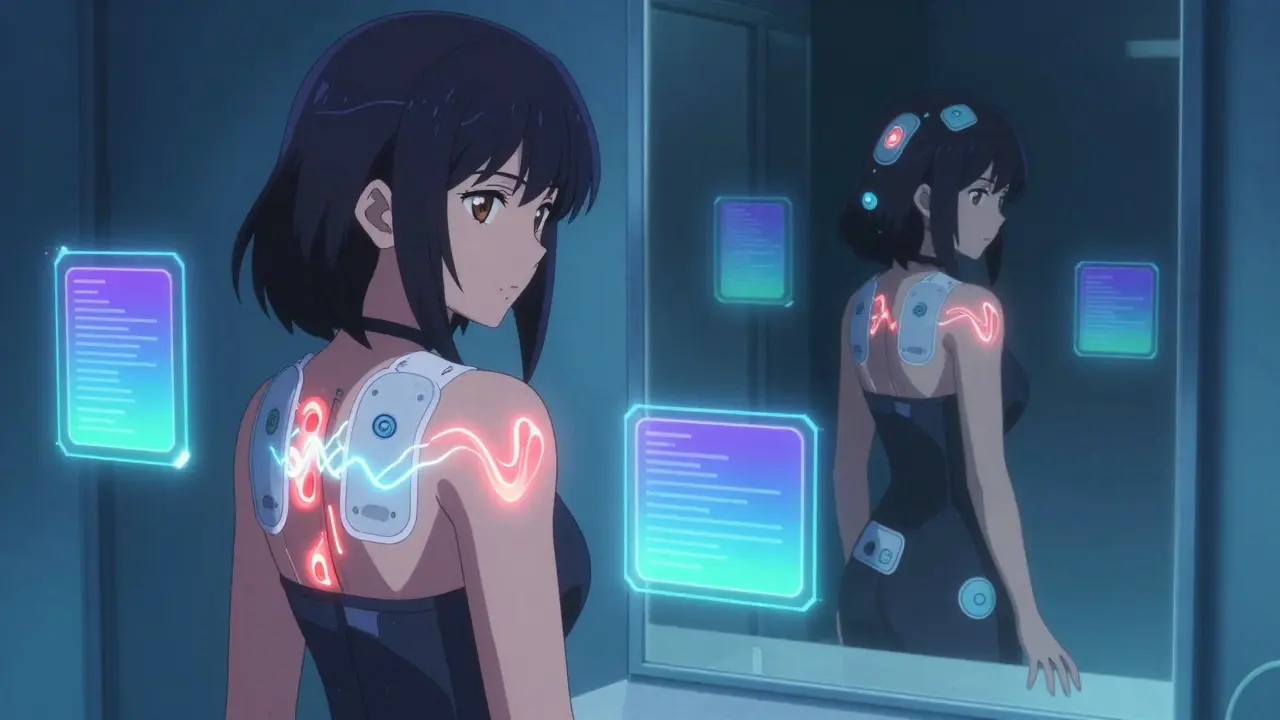
At Wake Forest University, Dr. Mohammad J. Moghimi and his team created a battery-free, wireless patch that sticks to your skin like a Band-Aid. It doesn’t take pictures. It measures bioimpedance-the way your skin conducts electricity. Cancerous tissue has different electrical properties than healthy skin. In a small trial with 10 volunteers, the patch detected differences with statistical significance (p<0.05). The goal? Let people wear it for days, track changes over time, and get alerts if something shifts. Imagine checking your skin the way you check your heart rate on a smartwatch.
Then there’s iToBoS, an EU-funded project with 20 research partners, including Fraunhofer Institute. Their full-body scanner takes 6 minutes to map every inch of your skin. It doesn’t just take photos-it builds a 3D map of every mole, spot, and freckle. Then, explainable AI (XAI) highlights which lesions are most concerning, and why. It doesn’t just say “cancer.” It shows you the exact texture, color gradient, and border irregularity that triggered the alert. Dermatologists in pilot clinics reported 78% satisfaction, but also a 35% false positive rate. That’s still too high. But it’s improving.
Immunotherapy: Turning Your Body Into a Cancer Fighter
If melanoma spreads beyond the skin, surgery alone won’t save you. That’s where immunotherapy changed everything. Before 2011, metastatic melanoma had a median survival of less than a year. Today, nearly half of patients live five years or more.
How? By unlocking your immune system. Melanoma tricks your body into ignoring it. Immunotherapy drugs like pembrolizumab (Keytruda) and nivolumab (Opdivo) block a protein called PD-1, which cancer uses to hide. Another drug, ipilimumab (Yervoy), targets CTLA-4, another immune brake. Used together, they’re even more powerful. In clinical trials, combination therapy led to durable responses in over 50% of patients.
But it’s not magic. Side effects can be brutal: fatigue, rash, diarrhea, even life-threatening inflammation of the liver or lungs. And not everyone responds. Only about 40-50% of patients see long-term benefit. That’s why researchers are now testing next-gen drugs. Regeneron’s fianlimab, which blocks LAG-3, is being tested alongside PD-1 inhibitors. Early results show deeper and longer-lasting tumor shrinkage.
And then there’s IMA203, a cell therapy in Phase 3 trials. It’s not a drug-it’s your own immune cells, trained in a lab to hunt down melanoma cells with a specific marker called PRAME. In Phase 1b, 56% of patients saw complete tumor disappearance. That’s not a typo. It’s a revolution.
Why Early Detection Isn’t Just About Saving Lives-It’s About Saving Treatment
Every year, thousands of people undergo surgery, radiation, or chemotherapy for melanoma that never would’ve spread. That’s overdiagnosis. A 2025 paper in Taylor & Francis warned that aggressive screening might lead to “excess morbidity with little survival benefit.” Think about it: if you get a biopsy for a harmless mole, you get a scar. You pay for it. You stress about it. And you might end up with an unnecessary surgery.
That’s why the best approach isn’t just “detect more.” It’s “detect smarter.” AI helps. Wearables help. But the real win is combining them with clinical judgment. A 2025 study in Expert Review of Medical Devices found dermatologists didn’t improve their accuracy with DermaSensor-they were already good. But primary care doctors? They improved dramatically. So the real value isn’t replacing experts. It’s empowering those who aren’t.
What You Can Do Right Now
You don’t need a scanner or an AI app to save your life. Here’s what works:
- Check your skin monthly. Use a mirror. Look at your back, scalp, between fingers and toes. Take a photo every 3 months so you can spot changes.
- Know your risk. Fair skin? Sunburns as a kid? Family history? Get checked yearly-even if you don’t see anything.
- If a spot changes in size, color, or texture in under 3 months, see a dermatologist. Don’t wait.
- Ask your doctor: Do you use dermoscopy? Are you trained on diverse skin tones?
- If you’re high-risk, ask about AI-assisted tools. They’re not everywhere yet, but they’re in most major clinics by 2026.
The Bottom Line
Melanoma is no longer a death sentence. But it’s still a race against time. The tools to catch it early are better than ever. The treatments to stop it from spreading are more powerful than ever. But none of it matters if you don’t look. If you don’t ask. If you don’t act.
One small spot. One quick visit. One decision. That’s all it takes to change your future.
Can melanoma be detected without a biopsy?
Some AI tools and devices like DermaSensor or full-body scanners can strongly suggest melanoma without a biopsy, but no non-invasive method is 100% reliable yet. A biopsy remains the only way to confirm a diagnosis. These tools help doctors decide which spots to biopsy, reducing unnecessary procedures-but they don’t replace them.
How accurate are AI skin cancer apps on smartphones?
Most consumer apps aren’t FDA-cleared and aren’t reliable. They often misclassify benign moles as cancerous-or worse, miss real melanomas. A 2024 study in The Lancet Digital Health found smartphone apps had accuracy rates between 60% and 80%, far below clinical-grade AI systems. Don’t rely on them. Use them only as a reminder to see a doctor, not as a diagnosis tool.
Is immunotherapy better than chemotherapy for melanoma?
Yes, for most patients with advanced melanoma. Immunotherapy has higher response rates, longer survival, and fewer side effects than traditional chemotherapy. Chemo rarely works on melanoma. Immunotherapy doesn’t kill cancer cells directly-it helps your body do it. That’s why it’s now the first-line treatment for stage III and IV melanoma.
Can melanoma come back after treatment?
Yes. Even after successful surgery or immunotherapy, melanoma can return-sometimes years later. That’s why lifelong follow-up is critical. Most doctors recommend check-ups every 3-6 months for the first 5 years, then annually. Skin self-checks are just as important. If you notice a new spot or a change in an old one, get it checked immediately.
Are these new detection tools available in New Zealand?
Yes, but access varies. Major hospitals in Wellington, Auckland, and Christchurch are beginning to use AI-assisted dermoscopy and handheld devices like DermaSensor. Full-body scanners are still mostly in research settings. Public health systems are evaluating them for wider rollout. If you’re concerned, ask your GP or dermatologist if they use any AI tools or if they can refer you to a clinic that does.
What’s Next?
The next five years will bring even more breakthroughs. Think blood tests that detect melanoma DNA floating in your bloodstream. AI that predicts your personal risk based on your genes, sun exposure, and skin history. Wearables that track mole changes in real time. The goal isn’t just to treat melanoma-it’s to stop it before it starts.
But none of that matters if you don’t take the first step. Look. Ask. Act. Your skin remembers every sunburn. Don’t let it be the only one keeping score.












Write a comment
Your email address will be restricted to us