
Fatigue in autoimmune disease isn't just being tired. It's the kind of exhaustion that makes brushing your teeth feel like climbing a mountain. You sleep eight hours, wake up refreshed in theory-but by noon, you're slumped over the kitchen counter, unable to lift a coffee cup. This isn't laziness. It's not poor sleep hygiene. It's a biological storm inside your body, and it's happening to nearly every person with an autoimmune condition.
Research shows 98% of people with autoimmune diseases experience this level of fatigue. That’s not a typo. In conditions like lupus, multiple sclerosis, and rheumatoid arthritis, fatigue isn’t a side effect-it’s a core symptom, often worse than pain or joint damage. A 2019 study across 15,000 patients found that 67% rated their fatigue as severe enough to stop them from working, caring for their kids, or even leaving the house. And here’s the kicker: standard rest doesn’t fix it. Sleep, naps, caffeine-they all fall short. That’s because this fatigue isn’t coming from your muscles. It’s coming from your brain.
Why Your Body Feels Like It’s Running on Empty
Autoimmune fatigue doesn’t work like regular tiredness. Normal fatigue fades after rest. This kind lingers for months, gets worse after tiny efforts, and doesn’t improve even when your disease seems under control. The reason? Inflammation. Not the kind you can see-swelling, redness-but invisible, deep inflammation in your nervous system.
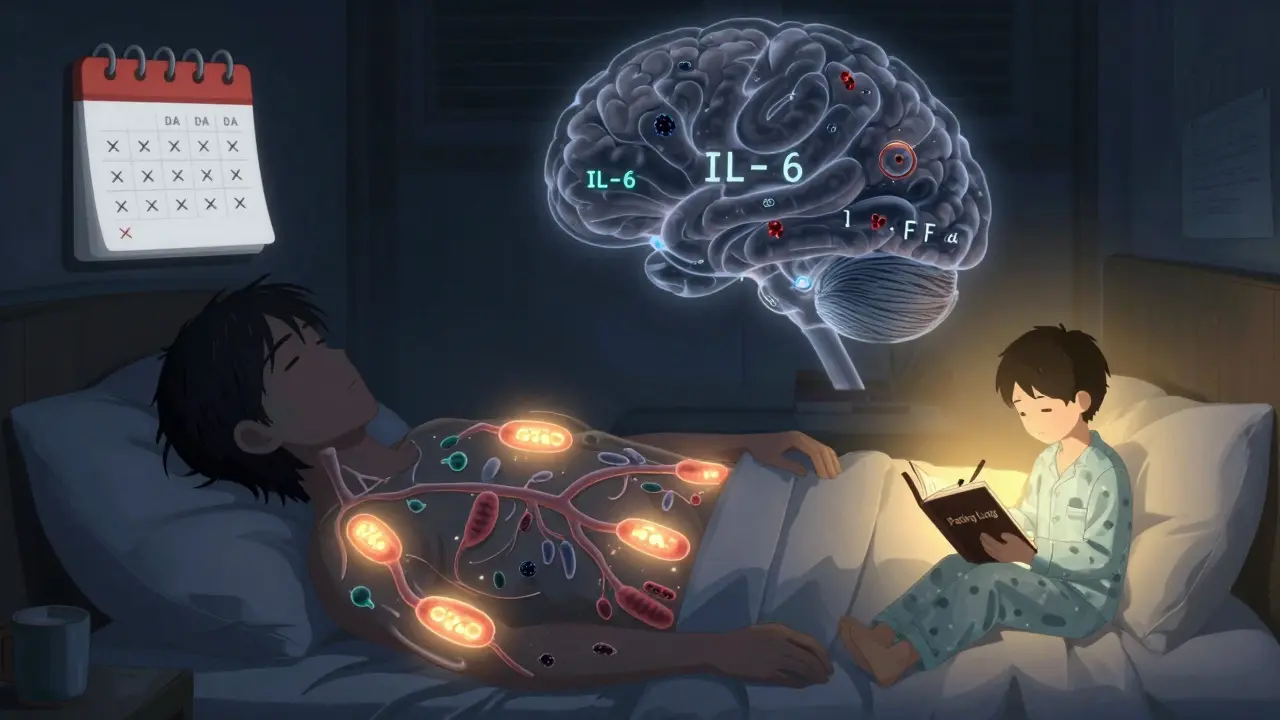
When your immune system attacks your own tissues (as it does in autoimmune diseases), it releases chemicals called cytokines-especially IL-1β, IL-6, and TNF-α. These aren’t just troublemakers in your joints or skin. They cross into your brain. Once there, they interfere with the circuits that control energy, motivation, and alertness. MRI scans show clear signs of brain inflammation in 82% of patients with severe autoimmune fatigue. It’s like your brain is stuck in slow motion, flooded with chemical smoke.
Another major player is your stress response system-the HPA axis. This is the part of your brain that tells your body how to handle stress by releasing cortisol. In many autoimmune patients, this system is damaged. Cortisol levels drop by 18-22% compared to healthy people. That means your body can’t ramp up energy when you need it. You’re not lazy-you’re running on a broken fuel line.
Then there’s your mitochondria. These are the tiny power plants inside every cell that make ATP, the energy currency of your body. In 65% of autoimmune fatigue cases, mitochondria are struggling. Muscle biopsies show 40-55% less ATP production. So even if your brain says “go,” your cells don’t have the fuel to move. This isn’t about being out of shape. It’s about cellular starvation.
How Fatigue Varies Across Autoimmune Conditions
Not all autoimmune fatigue is the same. It changes based on the disease, and knowing the pattern helps tailor treatment.
- Systemic Lupus Erythematosus (SLE): 98% of patients report fatigue. It often spikes with flares, but even when labs look normal, the exhaustion stays. Anti-dsDNA antibody levels correlate with fatigue severity-meaning your immune activity directly affects how drained you feel.
- Multiple Sclerosis (MS): 96% experience fatigue. In MS, it’s strongly linked to brain lesions in the thalamus, a region that controls alertness. Fatigue here can hit without warning, even on days when mobility is fine.
- Rheumatoid Arthritis (RA): 94% report fatigue, and for 63% of RA patients, it’s their #1 complaint-worse than joint pain. DAS-28 scores (a measure of disease activity) only partially explain it. Fatigue can be severe even with low inflammation.
- Sjögren’s Syndrome: 92% have fatigue, and 78% rate it as 8 or higher on a 10-point scale. This group often has the most debilitating fatigue, with brain fog so intense they forget names mid-sentence.
- Celiac Disease & Type 1 Diabetes: Even conditions you might think are “digestive” or “metabolic” come with fatigue. 90% of celiac patients and 88% of type 1 diabetics report chronic exhaustion, often linked to nutrient malabsorption and blood sugar swings.
And then there’s ME/CFS-Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. It’s increasingly seen as an autoimmune disorder. To be diagnosed, you need fatigue lasting six months, post-exertional malaise (symptoms crash 12-48 hours after activity), and unrefreshing sleep. 89% of ME/CFS patients also have another autoimmune condition. This overlap isn’t coincidence. It’s evidence that fatigue is a shared pathway.
What Doesn’t Work (And Why)
Many people try the obvious fixes: more sleep, caffeine, vitamins, or pushing through with exercise. But these often backfire.
Take caffeine. It might give you a 2-hour boost, but it disrupts sleep later, lowers cortisol even more, and can spike anxiety. Over time, it makes fatigue worse.
“Just exercise more” is another myth. Pushing too hard triggers post-exertional malaise-a crash where symptoms spiral for days. A 2021 Cleveland Clinic study found that 41% of patients who tried standard graded exercise therapy got worse, not better. The problem? Most programs don’t account for the unique energy limits of autoimmune fatigue. It’s not about building stamina. It’s about preserving what little energy you have.
And don’t assume your doctor will know. Only 12% of rheumatologists routinely use validated tools like the FACIT-F or MFI-20 to measure fatigue. Too often, it’s dismissed as “just stress” or “depression.” But this isn’t mental. It’s measurable. Your cytokines are elevated. Your cortisol is low. Your mitochondria are underperforming. This is biology-not psychology.

What Actually Helps: Evidence-Based Strategies
There’s good news: we now have tools that work. Not magic cures-but real, science-backed methods that help people reclaim their lives.
1. Pacing: Your New Superpower
Pacing isn’t laziness. It’s strategy. It means breaking tasks into tiny chunks, resting before you hit exhaustion, and listening to your body’s signals. One patient, Sarah, from Wellington, started doing 10 minutes of laundry, then sat for 20. Then 10 more minutes. She went from doing nothing all week to completing basic chores daily. Pacing has a 78% success rate in patient surveys. It’s the most effective tool because it stops the crash cycle.
2. Sleep Optimization
Fixing sleep isn’t about sleeping more-it’s about sleeping right. Autoimmune fatigue often comes with disrupted circadian rhythms. Melatonin production drops by 37%. Light exposure in the morning (even 15 minutes of natural light) resets your internal clock. Avoid screens after 8 p.m. Keep your bedroom cool. Use blackout curtains. Treat sleep apnea if you have it. Patients who follow a strict sleep routine see a 22-25% drop in fatigue.
3. Cognitive Behavioral Therapy for Autoimmune Fatigue (CBT-AF)
This isn’t talk therapy for depression. It’s a structured program that teaches you how to reframe fatigue, set realistic goals, and reduce fear of activity. A 2019 study showed CBT-AF improved fatigue by 27% more than standard care. It helps you stop feeling guilty for resting and start seeing rest as part of healing.
4. Targeted Supplements
Coenzyme Q10 (CoQ10) supports mitochondrial function. In trials, 200mg daily improved fatigue scores by 29%. Vitamin D deficiency is common in autoimmune patients-correcting it can reduce inflammation and boost energy. Omega-3s (EPA/DHA) lower IL-6 and TNF-α. Magnesium glycinate helps with sleep and muscle relaxation. Always test levels first. Don’t guess.
5. Medications (When Needed)
For some, medication makes a difference:
- Low-dose hydrocortisone (10-20mg/day): Only if you have proven HPA axis dysfunction. Helps restore cortisol rhythm. Not for everyone.
- Modafinil: Used in MS and lupus. Improves alertness in 28% more patients than placebo. Not a stimulant-it doesn’t cause jitteriness.
- Anti-IL-6 drugs (like tocilizumab): In early trials for RA and lupus, they reduced fatigue by 38%. Still experimental, but promising.
Combining these approaches is key. A 2021 Cleveland Clinic study of over 1,200 patients found that those who got integrated care-medication, CBT-AF, pacing, and sleep support-had a 45% greater reduction in fatigue than those on standard care. And 68% of them saw real, meaningful improvement.
What’s Coming Next
Researchers are racing to find better answers. The NIH just funded $18.7 million for fatigue-specific research. Three drugs are in final trials, with the first FDA-approved fatigue treatment expected by 2026. Blood tests to measure fatigue biomarkers (not just disease activity) are being developed. Soon, you might get a score that tells you how bad your fatigue is-objectively.
For now, the message is clear: Your fatigue is real. It’s not in your head. It’s in your immune system, your brain, and your cells. And there are ways to manage it-not cure it, but manage it-so you can live a full life again.
Is autoimmune fatigue the same as chronic fatigue syndrome (ME/CFS)?
They’re closely related but not identical. Autoimmune fatigue is fatigue caused by conditions like lupus or RA. ME/CFS is a distinct illness with its own diagnostic criteria-fatigue lasting 6+ months, post-exertional malaise, and unrefreshing sleep. But 89% of ME/CFS patients also have an autoimmune disease, and many experts now believe ME/CFS is an autoimmune disorder. The symptoms and management strategies overlap heavily.
Why doesn’t more rest help with autoimmune fatigue?
Because the problem isn’t lack of sleep-it’s how your body produces and uses energy. Your brain is flooded with inflammatory signals that block alertness. Your mitochondria can’t make enough ATP. Your cortisol rhythm is broken. Sleeping longer won’t fix these biological issues. In fact, too much bed rest can worsen muscle weakness and disrupt your circadian rhythm further. The goal isn’t to sleep more-it’s to sleep better and move smarter.
Can diet help reduce autoimmune fatigue?
Yes, but not because of one magic food. Anti-inflammatory diets (rich in vegetables, fatty fish, nuts, and olive oil, low in sugar and processed carbs) help reduce cytokine levels. For people with celiac or Hashimoto’s, removing gluten or dairy can cut fatigue by 30-40%. But diet alone won’t fix it. It works best when combined with pacing, sleep, and stress management. Avoid extreme diets-they can worsen nutrient deficiencies and increase fatigue.
Should I take supplements like CoQ10 or vitamin D?
Test first. Many autoimmune patients are low in vitamin D, magnesium, and CoQ10. Studies show 200mg of CoQ10 daily improves fatigue by 29%. Vitamin D correction can reduce inflammation markers. But don’t guess-get blood work. Taking too much vitamin D can cause toxicity. Too much CoQ10 can interfere with blood thinners. Always talk to your doctor before starting supplements.
Why do some doctors dismiss fatigue as psychological?
Because for decades, it was. In the 1980s and 90s, fatigue was often labeled as depression or anxiety, especially in women. But modern science has changed that. We now have MRI evidence of brain inflammation, blood tests showing elevated cytokines, and measurable drops in cortisol and ATP. The problem is that many doctors haven’t updated their training. Ask for the FACIT-F or MFI-20 fatigue scale. If they don’t know it, bring the tool yourself. You’re not overreacting-you’re advocating for real science.




















Write a comment
Your email address will be restricted to us